


RELIEVE KNEE PAIN, WALK WITHOUT PAIN
Knee pain is a frequent complaint that affects people of all ages. It can be the result of an injury, such as a torn ligament or a torn cartilage. Some diseases, such as arthritis, gout, and infections, can also cause knee pain.
Many types of mild knee pain respond well to self-care measures. Physical therapy and knee immobilization devices can also help relieve pain. However, in some cases, surgical repair may be necessary.
Knee pain symptoms may include:
-
Presence of swelling, pain, tenderness, temperature and visible bruising
-
Inflammation and stiffness
-
Redness and temperature to the touch
-
Weakness or instability
-
Clicking or cracking sounds
-
Inability to fully straighten the knee
Risk factor's
There are several factors that can increase the risk of knee problems, including:
-
Overweight
-
Lack of flexibility or muscle strength
-
Certain sports and occupations
-
Previous injury
How is knee pain treated?
During a physical examination, your doctor will likely recommend the following:
-
Inspec t ion of the knee for swelling, pain, tenderness, temperature, and visible bruising
-
Check how far you can move the lower leg in different directions
-
Push ing or pull ing the joint to assess the integrity of the knee structures
Behandlung
Treatments vary depending on the exact cause of the knee pain.
-
Medicines Medicines to relieve pain and and treat ment of pre existing conditions, such as rheumatoid arthritis or gout.
-
Strengthen ing of the muscles around the knee
-
Injections, always from th e hand of a specialist.
-
Surgery if you have an injury, you usually don't need to have surgery right away. Before making a decision decision, consider the advantages and disadvantages of both non surgical rehabilitation or surgical reconstruction, keeping in min d what is most important to you. If you choose surgery, the options include:
-
Arthroscopic surgery.
-
Partial knee replacement surgery.
-
Total knee replacement.
-
Internal compartment
-
External compartment
-
Retropatellar compartment
-
FEMORAL COMPONENT, which is the part that inserts into the lower part of the femur.
-
TIBIAL COMPONENT, which is attached to the upper part of the tibia
-
INSERT or INLAY, which is the polyethylene piece attached to the tibial component. It will act as the articular surface with the femoral component.
-
ROTULIAN COMPONENT or ROTULIAN BUTTON, which replaces the articular surface of the patella when the surgeon deems it necessary on a case-by-case basis.
-
INTERNAL or EXTERNAL FEMORAL COMPONENT, which is the part that inserts into the damaged lower femur.
-
INTERNAL or EXTERNAL TIBIAL COMPONENT, which is fixed to the upper part of the tibia
-
INTERNAL or EXTERNAL INSERT or INLAY, a polyethylene piece fixed to the tibial component. It shall act as an articular surface with the femoral component.
-
In the pre-anaesthesia room, the patient is prepared by inserting a peripheral venous line, administering the pre-operative antibiotic and, if necessary, shaving the surgical approach site.
-
In the operating theatre, the anaesthesiologist will administer sedation and spinal anaesthesia, so that the patient does not feel anything during the surgery. In rare cases, general anaesthesia may be used. The anaesthesiologist supervises the patient's condition throughout the operation by regulating and monitoring the patient's vital signs.
-
Once the patient has fallen asleep, a urinary catheter will be placed.
-
On the operating table, the patient will be positioned with the possibility to extend and flex the knee.
-
A longitudinal incision shall be made over the patella 15 cm long in case of total knee replacement or 10 cm long in case of partial knee replacement and deep enough to expose the joint.
-
The articular surfaces of both the tibia and femur of the knee will be exposed and following cutting guides customised to each knee and using a surgical saw, they will be cut. The size of the prosthesis will be determined and stability tests will be carried out.
-
After this check, the tibia and femur components shall be cemented and the insert shall be impacted into the tibial component.
-
After thorough washing of the surgical area, the wound is closed, leaving a drain to evacuate a possible haematoma.
-
Finally, the wound is covered with a sterile dressing and a compressive bandage and the patient is transferred to the resuscitation area until the anaesthesiologist determines when the patient can return to the inpatient ward.
-
The duration of the surgical procedure is approximately 30 minutes to one hour. The patient will be in the operating theatre area from the time he/she enters the pre-anaesthesia area until he/she leaves the resuscitation area when the anaesthesiologist indicates his/her transfer to the ward. Before being taken to the patient's room, a radiological control will be performed by the Radiology Department.
-
2-4 days in case of total knee replacement
-
2-3 days in case of partial knee replacement
-
Booking and use of the operating theatre.
-
Single room with accompanying bed. Food and hospitality for the patient.
-
Complete preoperative study.
-
Post-operative visits until medical discharge.
-
Medical fees.
-
Anaesthesiologist fees.
-
Fees for nursing staff.
-
Surgical material necessary for the operation.
-
Knee prostheses from ZIMMER & DePuy Synthes, world leaders in orthopaedics and traumatology.
-
Anaesthesia, haemotherapy-transfusions, recovery room booking, etc.
-
Medical complications insurance.
What does prosthetic knee surgery involve?
Total knee replacement involves the replacement of the articular surfaces of the knee with a metal prosthesis. The knee has excessive wear of its articular surfaces secondary to degenerative diseases or alteration of the load axis. This leads to a loss of mobility, constant pain and progressive deformity that in its evolution produces disabling pain with loss of quality of life.

In the knee joint we distinguish three compartments:
Occasionally in the knee only one of the three compartments is affected.
In such cases, only the articular surface of the damaged compartment is replaced, in which case the surgical procedure is less aggressive and recovery is quicker.
Surgical intervention in which only one joint surface or compartment of the knee is replaced is called partial knee arthroplasty. We distinguish between medial, lateral and retropatellar partial arthroplasty.
What does a knee prosthesis consist of?
The knee prosthesis replaces the original joint that is worn with loss of the articular surface.
The material used is stainless steel or cobalt or chromium alloys with a high density polyethylene intermediate component.
Components of total knee arthroplasty

Components of the partial knee arthroplasty:

Knee replacement surgery in Palma de Mallorca
Knee replacement surgery requires a protocol that is necessary for the safest and most successful procedure possible.
It is important in this first consultation that the patient provides all the information related to his or her case (X-rays, reports, MRI scans, etc.).
After the physical examination, the indication for total or partial knee arthroplasty will be decided whether or not.
In this first consultation, the patient will be able to ask all the questions he/she may have about the surgical procedure, in order to resolve any doubts and, in this way, make an informed decision about whether or not to undergo knee joint replacement surgery.
Once the decision has been made to carry out the total prosthesis operation in our PROST SURGERY UNIT, an appointment will be made for the preoperative study, as well as the corresponding consultation with our anaesthesiology specialist. Likewise, a date will be set for the surgical intervention.
Preoperative study with Dr. Fernando Muñoz
The tests to be performed in the preoperative study of the total knee replacement operation are an electrocardiogram, a complete blood analysis and a chest X-ray.
The next step is the visit with the anaesthesiologist, who will assess the patient's general condition, pathological history and the risk of anaesthesia, together with the complementary tests carried out. The type of anaesthesia to be applied during the operation will be determined.
Our team will give you preoperative instructions and teach you some breathing exercises to avoid intraoperative and postoperative problems.
Admission and knee replacement surgery
The patient will come to the clinic on the scheduled day. Admission will take place the night before, if the surgery is performed in the morning, or the same day if the hip replacement operation is performed in the afternoon.
Once the corresponding documentation has been handed over, the patient will be accompanied to his or her single room with an accompanying bed, where he or she will remain until the time of the operation. The patient will be showered with a special antiseptic gel and dressed in surgical clothes.
The total knee replacement operation step by step
Result of partial knee replacement surgery:
Before and After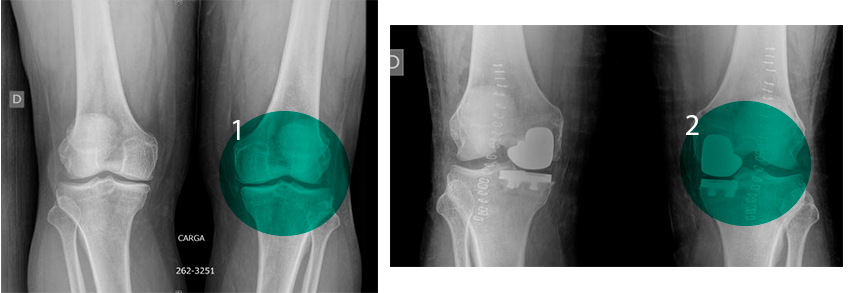
Result of total knee replacement surgery:
Before and After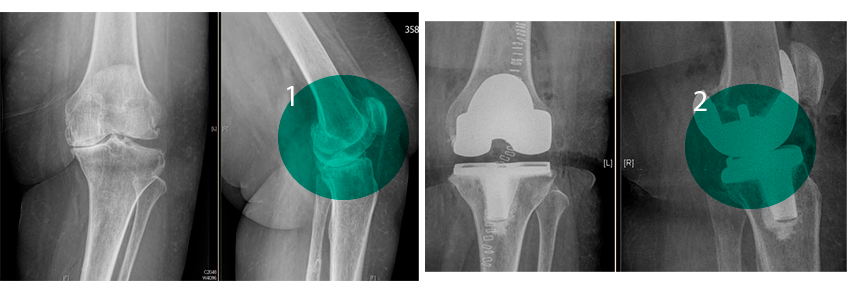
Recovery Phase
From the Radiology Department, the patient is transferred to his or her room on the hospital ward, where he or she will stay for 2 to 4 days in the case of total replacement, or 2 to 3 days in the case of partial replacement.
On the first day after surgery, a new control blood test will be carried out. In the rare case of a drop in haemoglobin, we will use the blood we have in reserve for each patient.
Also on this first day, the bladder catheter and drainage will be removed and the first treatment will be carried out.
From this first day after surgery, the patient will be mobilised with a walker or crutches, and this EARLY MOBILISATION is very important to avoid complications. The patient will be able to progressively load and move the joint.
The Physiotherapy Service will be responsible for teaching the patient to walk with crutches or a walker, so that, on the second or third day, the patient will be able to walk independently and can be discharged from hospital.
It is important to start movement and rehabilitation exercises as soon as possible, as this will significantly shorten recovery times, as well as the possibility of complications.
At home, the patient must continue with daily dressings of the surgical wound, so that after approximately twelve days the staples that close the wound can be removed.
Stay in the clinic:
Duration of surgery: 45 min-1 hour approximately.
Anaesthesia: Rachidian.
Knee prosthesis included: Yes
Full recovery: 3 to 6 months.
Price of a knee replacement operation in Palma de Mallorca
The price of the hip replacement operation by the Prosthetic Surgery Unit with Dr. Fernando Muñoz is closed.
The price for knee replacement surgery is all-inclusive. Below is an overview of what is included:
How long does it take to recover from knee surgery?
Regarding the time to return to work, it will depend directly on the type of work performed. In the case of a sedentary office job, the patient will be able to return to work around 2 months after the surgery, whereas if it is a job that requires significant physical effort, the waiting time can be extended to between 4 and 6 months.
As a general rule, the recovery time from knee arthroscopy depends on how long it takes for the inflammation caused by the surgery to disappear. The patient should follow
The patient should follow medial guidance such a s u sing crutches for as long as the specialist Doctor deems.